Auricular acupuncture, and the NADA protocol in particular, is often discussed in overly generalized or purely behavioral terms. A closer reading of the NIH-indexed review of the National Acupuncture Detoxification Association (NADA) protocol supports a more precise, neurophysiological interpretation that aligns well with contemporary evidence-based clinical practice.
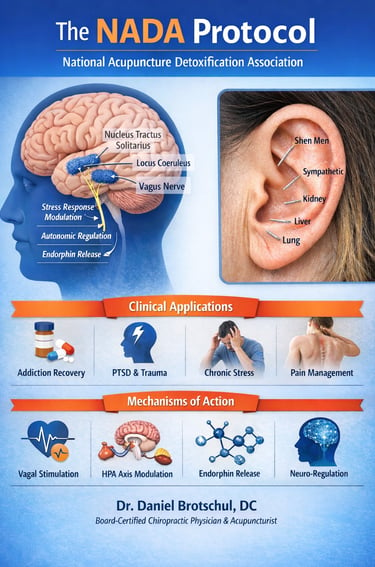
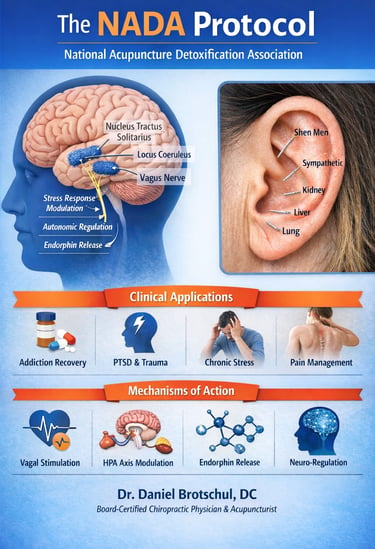
The NADA protocol consists of standardized bilateral stimulation of five auricular sites. From a neuroanatomical standpoint, the external ear represents a dense convergence zone of afferent input from the auricular branch of the vagus nerve, the trigeminal nerve, the facial nerve, and upper cervical spinal nerves. Mechanical stimulation via needling activates sensory afferents that project centrally to the nucleus tractus solitarius, locus coeruleus, and other brainstem structures involved in autonomic regulation, stress responsivity, and pain modulation.
The NIH review emphasizes that clinical outcomes associated with NADA—such as reductions in subjective distress, improved emotional regulation, and enhanced treatment engagement—are most consistently observed when the protocol is used as an adjunctive intervention rather than a stand-alone treatment. This is consistent with the broader neuromodulation literature, including medical dry needling, where therapeutic effects are mediated primarily through segmental and suprasegmental mechanisms rather than local tissue change alone.
Importantly, the authors frame NADA within an evidence-informed model that does not rely on traditional meridian theory. Instead, observed effects are attributed to well-established pathways involving autonomic balance, hypothalamic–pituitary–adrenal axis modulation, and central pain processing. This places the protocol conceptually alongside medical dry needling and other peripheral sensory stimulation techniques that leverage neuroplastic and regulatory mechanisms.
Methodological critiques—particularly regarding blinding and heterogeneity of outcome measures—are acknowledged in the review. However, the authors note that such limitations are common to many non-pharmacologic neuromodulatory interventions and do not negate consistent signals related to safety, feasibility, and clinical utility when NADA is integrated into comprehensive care models.
In our clinic, the NADA auricular protocol is offered within a broader framework that includes chiropractic care, acupuncture, and medical dry needling. It is applied selectively in patients where autonomic dysregulation, heightened stress reactivity, trauma exposure, or maladaptive pain processing are central features of the clinical presentation. Used this way, NADA functions not as an alternative therapy, but as a targeted neuromodulatory intervention consistent with contemporary evidence-based reasoning.
Dr. Daniel Brotschul, DC
Board-Certified Chiropractic Physician & Acupuncturist
DLUXESPA
3443 W Irving Park
Chicago, IL 60618
drjointmaster.com
(773) 356-5660
BY APPOINTMENT ONLY
© The Joint Master Chiropractic, All rights reserved.